Recognizing carpal tunnel symptoms before they escalate
It often starts as a faint “pins and needles” feeling that shows up only after a long stretch of typing, gripping a tool, or holding a mouse—then disappears before you can decide whether it was real. Because it comes and goes, it’s easy to write off as overuse or a strange sleeping position, especially when the hand looks normal and still feels strong most of the day.
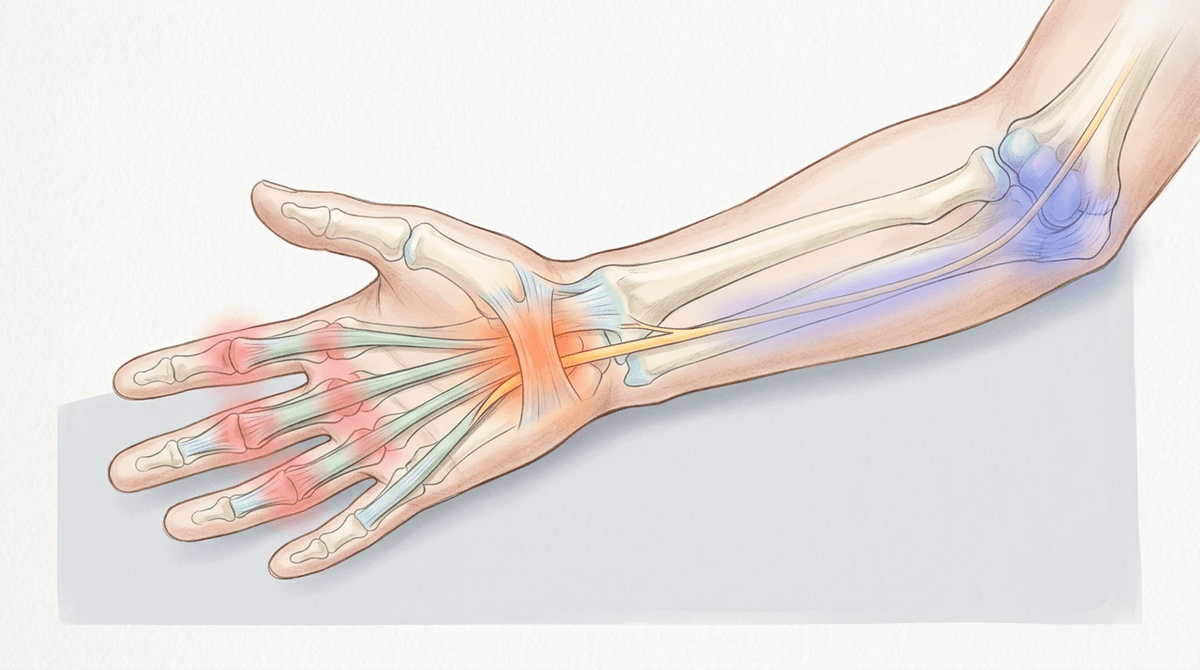
When the median nerve is getting crowded, the earliest clues are usually sensory and slightly inconsistent: tingling or numbness that favors the thumb, index, middle finger, and half of the ring finger, or a hand that feels oddly “puffy” even when it isn’t swollen. People often notice they’re shaking the hand out, rubbing the palm, or swapping grips without thinking—small, effortful workarounds that can become a pattern.
Over time, those brief episodes may last longer or show up more predictably with bent-wrist positions, repetitive finger motion, or sustained pressure through the heel of the palm. One reason this can creep forward is that rising pressure inside the carpal tunnel can reduce blood flow to the nerve and mechanically irritate it; a nerve under that kind of stress may start firing “false alarm” signals more easily, so sensations linger even after the task stops.
Why symptoms feel worse at night and waking

You might notice it most when everything is finally quiet: you roll over, your hand feels thick or “asleep,” and the tingling is sharp enough to wake you. By morning, it can be oddly inconsistent—better after a few minutes of shaking out the fingers, then flaring again as soon as you hold a toothbrush, phone, or steering wheel.
At night, the wrist often drifts into a bent position without you realizing it. That bend can narrow the carpal tunnel space, and when the tendons inside are already a bit reactive from the day’s work, even a small change in position may raise pressure enough to bother the median nerve. Lying down can also shift fluid toward the hands, which may add a subtle “crowded” feeling inside the tunnel, even when the skin doesn’t look swollen.
Waking symptoms can feel disproportionate because a compressed nerve doesn’t just “turn off”—it can become more electrically irritable. Reduced blood flow and sustained mechanical squeeze overnight may prime the nerve to misfire, so the first movements in the morning register as pins-and-needles instead of normal touch. If that pattern keeps repeating, people sometimes start sleeping more lightly, half-listening for the next flare, which can make the whole cycle feel harder to interpret.
What drives median nerve compression beneath the surface
Sometimes it’s not the tingling that stands out first, but a quiet sense that the hand is “full” or slightly stiff, even though you can’t see swelling. That mismatch can be confusing. The space the median nerve travels through is fixed on top by a firm band of tissue, so it doesn’t have much room to negotiate when anything inside runs a little bigger than usual.
After hours of finger motion and gripping, the flexor tendons can become more hydrated and their lining can thicken slightly, especially if they’ve been irritated repeatedly. Add a bent-wrist position—flexed or extended—and the tunnel volume drops while the contents push back. Pressure rises, blood flow to the nerve may dip, and the nerve can start sending noisy sensory signals that feel inconsistent with what your hand is actually doing.
When that squeeze happens again and again, the nerve may become easier to “set off,” so smaller triggers start to count: a brief hold on a phone, a short drive, a light tool grip. This shift can feel unfair—like symptoms are spreading without a clear cause—because the change is often in the nerve’s sensitivity as much as the task itself.
The confusion between carpal tunnel and lookalikes
It can throw you off when the tingling doesn’t follow the “rules”—maybe it creeps into the pinky, or the whole hand feels strange after a long day, not just the thumb-side fingers. That kind of overlap is common, and it’s one reason people bounce between “it’s my wrist” and “it must be my neck,” especially when symptoms shift hour to hour.
Some lookalikes change the map of sensation. Irritation of the ulnar nerve (often closer to the elbow or at the wrist) can pull in the ring and pinky fingers, while finger-joint or tendon inflammation can create aching and stiffness that feels like nerve trouble even when it’s more about irritated tissue. Sometimes the “hand is asleep” feeling is less about one nerve being squeezed and more about how tightly you’ve been gripping—muscles stay braced, circulation runs a little lower, and the brain reads that dull input as numbness.
Another complication is that a sensitized median nerve may start reacting outside the classic pattern, especially after repeated night flares. That can make quick self-tests and assumptions unreliable: a single odd day can look like proof you guessed wrong, even when it’s really inconsistency in how the nervous system is responding.
Risk factors that quietly load the wrist tissues
It can be surprisingly hard to connect the flare to anything you did, because the load often builds in small, boring ways—an extra week of deadlines, longer gaming sessions, a new tool with a thicker handle, or a stretch of driving where your wrist stays slightly bent. None of it feels “injury-level” in the moment, so the tingling can seem like it arrived out of nowhere.
What tends to matter is how often the tunnel gets asked to work in a narrowed, crowded state. Repetition and sustained gripping can leave the flexor tendons a little thicker and more fluid-rich, so they take up more space. Bent-wrist postures (both flexion and extension) reduce the tunnel’s volume, and contact pressure through the heel of the palm can add another squeeze. In some people, whole-body factors that shift fluid—like thyroid changes, or poorly controlled blood sugar—may make that “crowded” baseline more likely, even if hand use hasn’t changed much.
You might feel fine while working because adrenaline and attention blunt the signals, then notice the symptoms later when the nerve is more reactive and the tissues are still a bit swollen. That delay can lead to misinterpretation—blaming sleep alone—when the day’s accumulated pressure is still part of what the nerve is responding to.
How treatments reduce pressure versus calm nerve sensitivity
A splint can feel almost too simple—until you notice that the same hand that tingled all night is quieter when the wrist stays closer to neutral. That’s the “pressure” side of treatment: changing wrist angle and reducing repeated tendon glide can lower how crowded the tunnel gets, even if the tendons are still a little thick from daily use. The catch is that it can feel awkward or restrictive, and some people abandon it before they’ve had enough nights in a row to tell what it’s really changing.
Other options can seem to work in a different way, and that’s where the experience gets confusing. Steps aimed at inflammation or fluid-related swelling (sometimes including a corticosteroid injection) may reduce how much space the tendon tissues take up, so the nerve has more breathing room. But when the nerve has been “on alert” for a while, relief can lag or come in fits and starts—not necessarily because nothing helped, but because a sensitized nerve may keep misfiring even after the mechanical squeeze is partly improved.
Surgery, when it’s recommended, is mainly about creating lasting space by releasing the tight roof of the tunnel. People often expect an immediate reset, yet early soreness and residual tingling can coexist for a bit, which can be unsettling. If numbness keeps progressing or weakness starts to show up, that’s usually a cue to get the timing and the underlying driver re-checked rather than trying to outwork it.
When reasonable fixes cause unexpected discomfort or doubt
The first night a splint keeps your wrist straight, you might wake up with a different problem: a sore thumb base, a stiff forearm, or a pressure point along the palm that wasn’t there before. That can feel like a sign you chose the wrong fix, especially when the tingling still shows up anyway—just shifted, dulled, or arriving later than usual.
Part of the mismatch is mechanical. Holding the wrist near neutral changes which tissues take the load, and if the splint is snug, it can add contact pressure to an area that’s already touchy from daytime gripping. At the same time, a median nerve that’s been irritated for weeks may not “settle” on the same schedule as the pressure change; it can stay electrically jumpy for a while, so sensations come and go in a way that’s hard to read.
The uncertainty often peaks when symptoms change shape instead of disappearing—less night waking, but more daytime buzzing; less tingling, but a dull numb patch; less hand “asleep,” but more ache in the wrist. If numbness becomes more constant, or you start noticing dropping objects or thumb weakness, it’s usually worth getting reassessed rather than assuming you just need to push through.