The neck pain pattern that prompts action
It often starts as a familiar “stuck” feeling when you turn your head, then shows up again after a long stretch of screen time or a night where your pillow felt fine—until it didn’t. The frustrating part is the inconsistency: one day a quick walk loosens things up, the next day the same routine seems to end with a deeper ache at the base of the skull or a tight band into the top of the shoulder.
A pattern that tends to matter is when the discomfort becomes position-linked instead of purely “sore.” Sitting with your head slightly forward, looking down at a laptop, or holding a phone at chest level can gradually increase pressure on the disc and the small facet joints in the neck. As those tissues get irritated, nearby muscles may tighten to stabilize the area, which can feel protective in the moment but also makes motion feel more restricted—and can make the pain feel bigger than the original trigger.
People often notice the shift from local stiffness to symptoms that are harder to ignore: tingling that comes on in the arm after a certain posture, headaches that cluster around the same days as neck flares, or pain that reliably spikes with one movement (like looking over a shoulder while driving). None of that automatically signals something dangerous, but when symptoms become repeatable—showing up with the same positions, lasting longer, or taking more effort to “settle”—it’s usually a sign the irritation cycle is gaining momentum rather than resetting on its own.
What drives degeneration and irritation beneath the surface
You might notice the neck doesn’t just feel “tight” anymore—it feels a bit compressed, like you need to keep shifting to find a neutral spot, and even then it doesn’t fully settle. That extra effort to get comfortable often shows up before anyone thinks about structure, especially when the flare seems out of proportion to what you did that day.
Under the surface, the typical story is less about one “bad” posture and more about accumulated load over time. Cervical discs tend to lose water content as the years go on, which can reduce their ability to spread force evenly. When that cushioning changes, more stress may shift into the small facet joints behind the disc and the surrounding ligaments. Those tissues can get mechanically irritated, and the nervous system may respond by increasing muscle tone in the area—useful for short-term stability, but it can also make the neck feel guarded and stiff in a way that’s hard to stretch out.
As the cycle repeats, the body may lay down extra bone around joint margins as a kind of reinforcement. Many people have these changes without much pain, but on days when sleep support is off, screen time runs long, or stress keeps muscles “on,” the already-narrower spaces for nerves can feel less forgiving, and symptoms may become easier to trigger.
Why symptoms travel into shoulders and hands
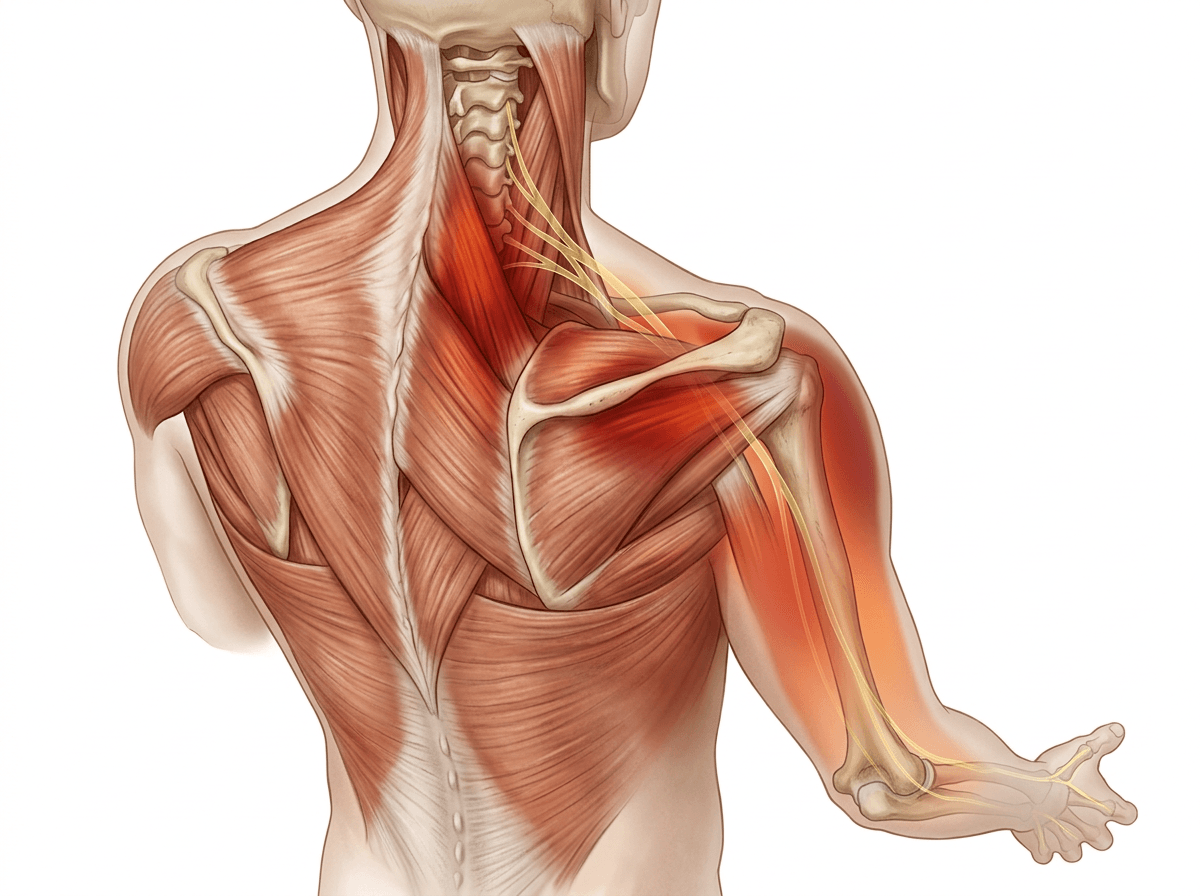
It can be subtle at first: your neck feels “fine enough,” but your shoulder starts to burn or your hand feels a little prickly after the same stretch of laptop time. The confusing part is how indirect it seems—like the neck is quiet while the arm gets all the attention—so it’s easy to blame the wrist, the shoulder, or a “bad knot” that won’t release.
One reason symptoms can travel is that the nerves that supply the shoulder, arm, and hand exit the spine through small openings between the vertebrae. When disc height is reduced or nearby joints and soft tissues are irritated, those openings may become less tolerant of certain positions—especially prolonged forward-head posture, repeated looking down, or sleeping with the neck rotated. In those moments, the nerve doesn’t have to be “damaged” to complain; even mild mechanical pressure or chemical irritation around the nerve root can change how it signals, which may feel like tingling, buzzing, or a dull ache that follows a partial pathway rather than staying in the neck.
Muscles around the neck and shoulder blade can tighten in a protective way, which can refer pain into the upper arm and create the impression that the problem is local. Meanwhile, on higher-load days, the same nerve pathway may act more sensitive overall, so smaller triggers—like holding the phone, reaching forward, or driving with the head turned—can feel surprisingly “too much,” even if the neck pain itself hasn’t spiked.
Is it safe to wait, or escalate now
Sometimes the deciding moment isn’t the pain—it’s the way you start managing your day around it. You catch yourself avoiding checking blind spots, propping your elbow just to keep hand tingling down, or waking up and needing a few minutes before your neck will “agree” to move. That kind of workaround can feel reasonable, but it also makes the situation harder to read because temporary relief doesn’t always mean the underlying irritation has settled.
Waiting often feels safest when symptoms are clearly position-linked and predictable: they ramp up with long looking-down stretches and ease when you change posture or activity. In those cases, the nervous system may simply be reacting to repeated mechanical stress—nerve tissue and nearby joints get sensitized, muscles tighten to stabilize, and the whole area becomes easier to provoke for a while. The trade-off is uncertainty: if the pattern is trending toward longer-lasting tingling, spreading numbness, or noticeable weakness, that can suggest the nerve has less “buffer” than it used to and deserves a faster check-in rather than more time.
More urgent evaluation is usually worth considering if you notice new or progressive arm or hand weakness, trouble with fine motor tasks, significant gait or balance changes, or bowel/bladder changes. Even when nothing dramatic is happening, symptoms that stop behaving like your usual flare—staying constant at rest, escalating quickly, or not easing after several days—are often the point where escalation becomes the more practical next step.
Lifestyle changes that lower mechanical load reliably
The first clue a change is doing something is usually mundane: you get to the end of a work block and realize you didn’t have to keep “resetting” your neck every few minutes. That’s different from the quick relief you can get from stretching, because the issue here is often cumulative load. When the head is carried even slightly forward for long periods, the extensor muscles in the back of the neck work overtime and the facet joints can take more compression. Over hours and days, that can leave the whole area more reactive, so smaller triggers start to feel bigger.
The more reliable lifestyle shifts tend to be the ones that reduce how long you stay in the same end-range position—especially chin-forward, eyes-down. Monitor height, laptop use, and phone habits matter less as “perfect posture” and more as time-under-tension. It’s also common to misread effort as progress: holding a rigid “upright” pose can increase muscle tone and make symptoms feel sharper, even though the intention is good.
Sleep can be the hidden multiplier. A pillow that lets your neck sag into side-bend or rotation for hours may narrow already sensitive spaces and you only notice it when you wake up stiff, foggy, or with arm tingling that takes time to fade. If a change consistently reduces that morning ramp-up over a week or two, it’s usually doing more than a temporary distraction.
Exercise therapy: helpful, but easy to misapply

The telltale sign exercise is helping is rarely a dramatic “fix.” It’s more like you finish a workday and notice the flare took longer to start, or the morning stiffness clears with less negotiation. But it can also go the other way: the same routine that felt good last week suddenly leaves you with a hotter neck, a heavier headache, or a faint return of arm tingling, which makes it hard to know whether you’re strengthening the right thing or just poking a sensitive system.
A lot of that comes down to load dosing. With age- and load-related changes, the neck can have less tolerance for sustained compression or end-range positions. Some exercises unintentionally recreate those positions—repeated chin pokes, aggressive extension, long holds done while already fatigued—so tissues that are already irritable get more pressure and the nervous system responds by tightening muscles further. That “guarding” can feel like weakness or stiffness that needs more stretching, when in some cases it’s the body trying to reduce motion because the area feels less buffered.
What tends to separate useful from irritating work is how your symptoms behave afterward, not how hard you worked in the moment. If a session reliably ramps symptoms for hours, or makes your usual triggers easier to set off the next day, that’s information—even if the movements look correct on paper.
Medications, injections, and manual care trade-offs
You can sometimes tell you’re reaching for “something stronger” when the usual resets stop working and the neck feels louder with fewer triggers. That’s often when over-the-counter pain relievers, anti-inflammatories, or muscle relaxers start to feel tempting—not because they fix the pattern, but because they can turn down the volume enough to get through a workday. The trade-off is misinterpretation: when pain is dampened, it’s easier to sit longer in the same positions that were loading the area in the first place.
Injections can create a different kind of relief—sometimes more targeted—by reducing inflammation around irritated joints or nerve roots. When they help, it may be because a calmer chemical environment makes a sensitive nerve fire less easily, even if the mechanical “space” hasn’t changed. The uncertainty is that response varies: some people get a meaningful window to move more normally, others feel little change, and a few feel briefly more sore as tissues react to the procedure.
Manual care (massage, mobilization, manipulation) often feels convincing because it changes sensation quickly—less guarding, more rotation, a lighter head. But that immediate shift can be short-lived if the nervous system was tightening muscles to protect an irritated segment; once you go back to the same loads, the body may re-create the tension. If symptoms start traveling more into the arm afterward or feel less predictable, that’s usually a sign to pause and reassess rather than pushing for “more release.”
When imaging and surgery become part of management
It’s often the moment the symptoms stop behaving like “your usual flare” that imaging comes up—when tingling doesn’t fade with position changes, sleep starts reliably provoking it, or weakness makes ordinary tasks feel uncertain. At that point, the question shifts from “what calms this down?” to “what, exactly, is being irritated, and where?”
Imaging can be clarifying, but it can also be oddly unsatisfying. Degenerative findings (disc height loss, joint overgrowth) are common even in people who aren’t hurting, so a report may read “worse” than you feel—or miss why a specific posture triggers symptoms. The value is in matching pictures to a pattern: persistent nerve-root signs, suspected spinal cord involvement, or symptoms that aren’t following the usual cycle.
Surgery typically enters the conversation when the cost of waiting seems higher than the risk of intervening—especially with progressive weakness, clear cord-related changes, or pain/tingling that stays intrusive despite time and well-matched care. Even then, decisions can feel uncomfortable because “fixing compression” doesn’t always map neatly to how sensitized the system has become, so it’s worth treating a fast change in strength or coordination as a reason to be seen sooner rather than later.











