The common expectation: hardware comes out eventually
It’s often a surprise how “present” the hardware can feel once the big pain is gone—like a firm edge under the skin, a tight spot when you kneel, or an ache that only shows up in cold weather. That sensation can make removal sound like the obvious end point, almost like stitches that are simply waiting to come out. But that expectation isn’t always aligned with how fixation is meant to work.
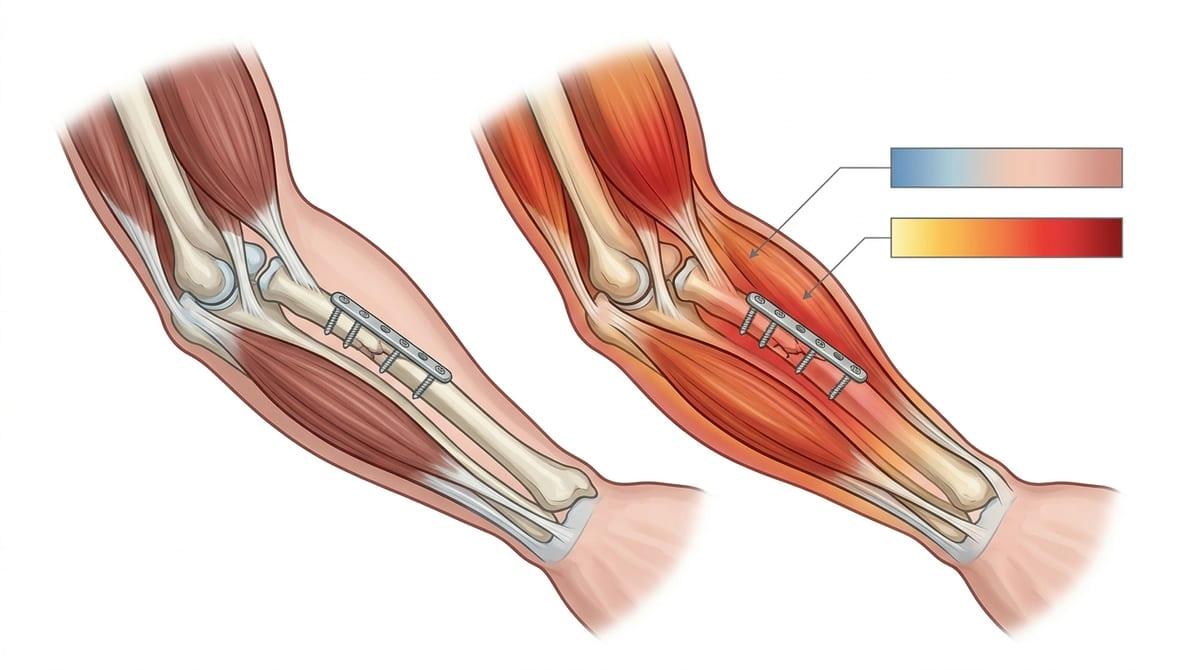
Plates and screws are typically designed to stay in unless they create a specific problem. Early on, they share load with bone while healing is still inconsistent—strong in some areas, weaker in others—so the implant acts like a quiet backup during everyday stress. Later, as swelling fully settles and you move more, the same metal can become easier to notice: less padding over it, more tendon glide across it, and more “feedback” from pressure points. That shift can feel like something is wrong, even when the bone itself is doing fine.
A person can feel ready because function is mostly back, while the bone is still remodeling in the background—and those two don’t always match. That mismatch is often where the “it must come out eventually” idea takes hold, even before anyone has confirmed that taking it out would actually reduce symptoms.
Why removal can feel urgent, even without danger
It can start as a small, oddly specific annoyance—your skin catches on a seatbelt, a shoe collar presses right where a screw head sits, or a single yoga pose suddenly feels “impossible” again. Even when everything looks stable on an X-ray, that daily friction can create a sense that something is actively wrong, because your brain treats repeatable, localized discomfort as a problem that needs a clear endpoint.
Part of the urgency is mechanical: as swelling and protective stiffness fade, the hardware may become more exposed to pressure and motion from nearby tendons, fascia, or thin skin. The bone can be healed and still be remodeling, while the soft tissues are doing their own adapting—sometimes inconsistently—so symptoms can spike on high-use days and then quiet down, which is confusing. That pattern often gets interpreted as “the metal is rejecting,” when it may simply be a sensitive interface that’s now easier to provoke.
Once you’re active again, every reminder of the implant can feel like it’s blocking the “final step” back to normal. That perception can make removal feel urgent even without red flags, because the discomfort is predictable, hard to ignore, and doesn’t behave like a typical healing ache.
What drives irritation around plates and screws
Sometimes it’s a sharp “pinch” only at one angle, or a dull pressure that shows up after a long walk and then disappears the next day. That inconsistency can make it hard to trust your own read on what’s happening, especially when the area looks calm and the fracture site itself doesn’t feel unstable.
A big driver is simple contact mechanics. As post-op swelling fully resolves and muscle tone changes with returning activity, there may be less soft-tissue cushion over a plate or screw head—especially in superficial spots like the ankle, clavicle, wrist, or the front of the shin. With certain movements, tendons and fascia can glide repeatedly over a raised edge, and the body may respond with localized inflammation that feels like “metal irritation,” even though it’s often the soft tissue that’s getting irritated.
Another factor is micromotion at interfaces. Even after union, tiny shifts between hardware and bone (or between screw and plate) can transmit stress to the periosteum and nearby nerve endings. Cold sensitivity can also amplify the sensation, not because the implant is “reacting,” but because colder tissues tend to be stiffer and less forgiving under pressure.
Why taking hardware out can create new problems
The first few days after removal can feel oddly “raw,” even when the original deep ache is gone—like the area is unprotected. That’s partly because the hardware wasn’t just sitting there; it was changing how force traveled through the bone and nearby soft tissue, and your body had adapted to that pattern.
Once screws come out, the bone is left with temporary voids where the threads were. Even with confirmed union, those holes can act like small stress risers until they fill in, which can make heavier activity feel more precarious than expected. At the same time, the surgeon often has to dissect through scar tissue that formed around the plate and screw heads. That scar can tether nerves or tendons, so separating it can irritate structures that weren’t causing symptoms before, and the result may be new numbness, tendon soreness, or a different kind of pain.
If the main driver was soft-tissue sensitivity or cold-related stiffness, removal may help, but it doesn’t always reset those responses right away. If you’re weighing timing, it helps to treat removal as a new procedure with its own recovery, not just an “undo.”
Clear reasons to remove versus reasons to wait
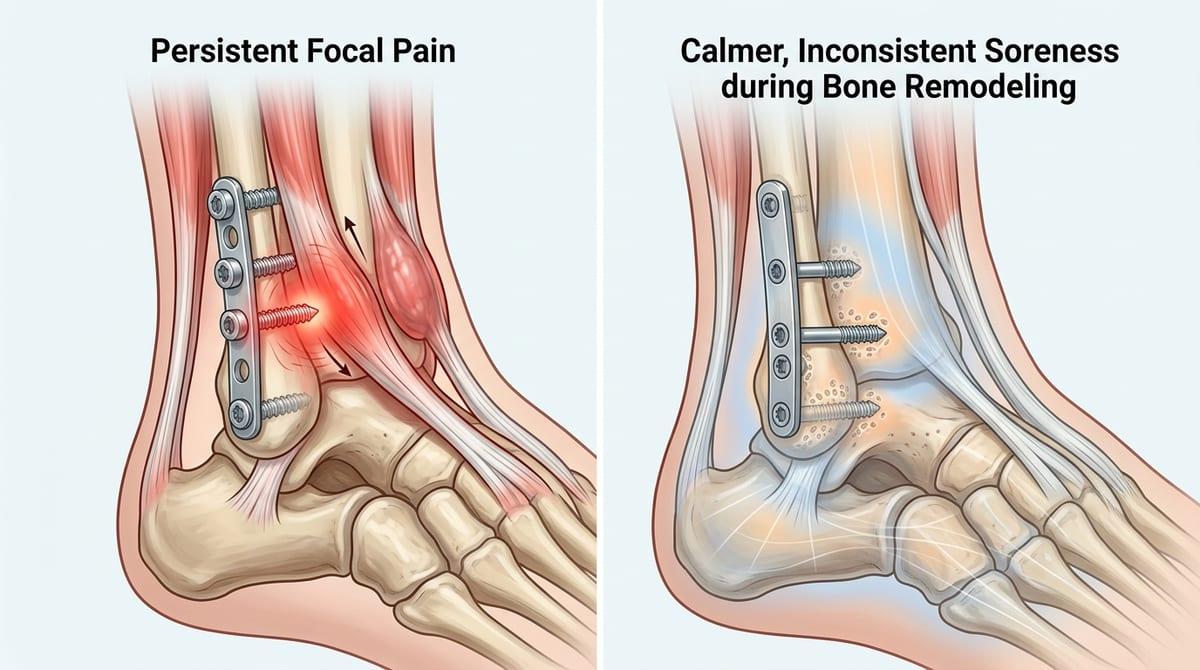
It’s telling when the discomfort stops being “background” and turns into a repeatable, map-able problem—one screw head that always rubs in boots, a plate edge that you can’t kneel on, a zip of pain when a tendon slides over one spot. In those cases, removal is often discussed because the symptom has a clear mechanical trigger, not just a vague ache. More urgent reasons tend to be less subtle: drainage, escalating warmth and swelling, a wound that won’t settle, or pain that’s paired with new numbness or catching that suggests a nerve or tendon is being bothered.
Waiting usually makes sense when the main issue is inconsistent soreness that flares with load, then calms down, especially if the bone is still in the phase where it’s remodeling and strength is uneven. The trade-off is that “feeling fine” isn’t the same as “ready for holes from screws,” and confirmed union matters because the implant may still be sharing force in ways you don’t feel day to day.
Cold sensitivity, skin tenderness, and end-of-day throbbing can fade as tissues toughen and scar becomes less reactive—yet they can also persist if the hardware is prominent or superficial. That uncertainty is why the same complaint can lead to opposite recommendations, depending on location, activity demands, and what imaging suggests about how much protection the bone still needs.
A reasonable choice that backfires: early removal
It often feels like a clean, sensible decision: you’re back to work, back to training, and the only thing that still “talks” is the plate. The discomfort is specific, predictable, and you can point to the exact edge that rubs—so taking it out early can sound like closing the loop. The catch is that comfort and structural readiness don’t always line up, and that mismatch is easy to underestimate.
Even when union looks solid, the bone may still be unevenly strong as it remodels, and the implant may still be sharing load in ways you don’t notice until it’s gone. Removing screws leaves temporary holes that can concentrate stress, and early on those weak spots haven’t had much time to fill in. In active people, the “backfire” is usually timing: the area feels better quickly, then a return to impact or twisting loads exposes how much the hardware was quietly buffering—sometimes as new pain, sometimes as a setback that forces another pause.
Questions that clarify timing for your surgeon
It’s frustrating when the area feels “good enough” most days, but one movement or one piece of gear reliably finds the same sharp spot. That’s usually the moment where timing questions matter more than the generic idea of “removal,” because two people can have the same symptoms while the underlying load-sharing and soft-tissue irritation are in very different phases.
Useful questions tend to separate bone readiness from symptom drivers: “Has union been confirmed on the views you trust, and is there any reason you think the implant is still protecting a weaker zone?” “Is my pain more consistent with tendon or nerve irritation over prominent hardware, versus stress through the bone?” “If screws come out, how long do the thread holes act like stress risers for my sport, and what activity would be the first real test?”
It also helps to ask about the practical uncertainty: “If we wait 3–6 more months, what changes would make removal more or less likely to help?” and “What’s the specific downside of leaving it in for now in this location?” If the answers stay vague, that’s often a cue to slow the decision down rather than speed it up.