Why shoulder blade pain can shoot into the arm
It often starts as a dull spot under the shoulder blade—then, on a long drive or a heavy carry, the feeling seems to “spill” into the upper arm or even the hand. That spread can be confusing, especially when the shoulder blade itself is what feels sore and tender.
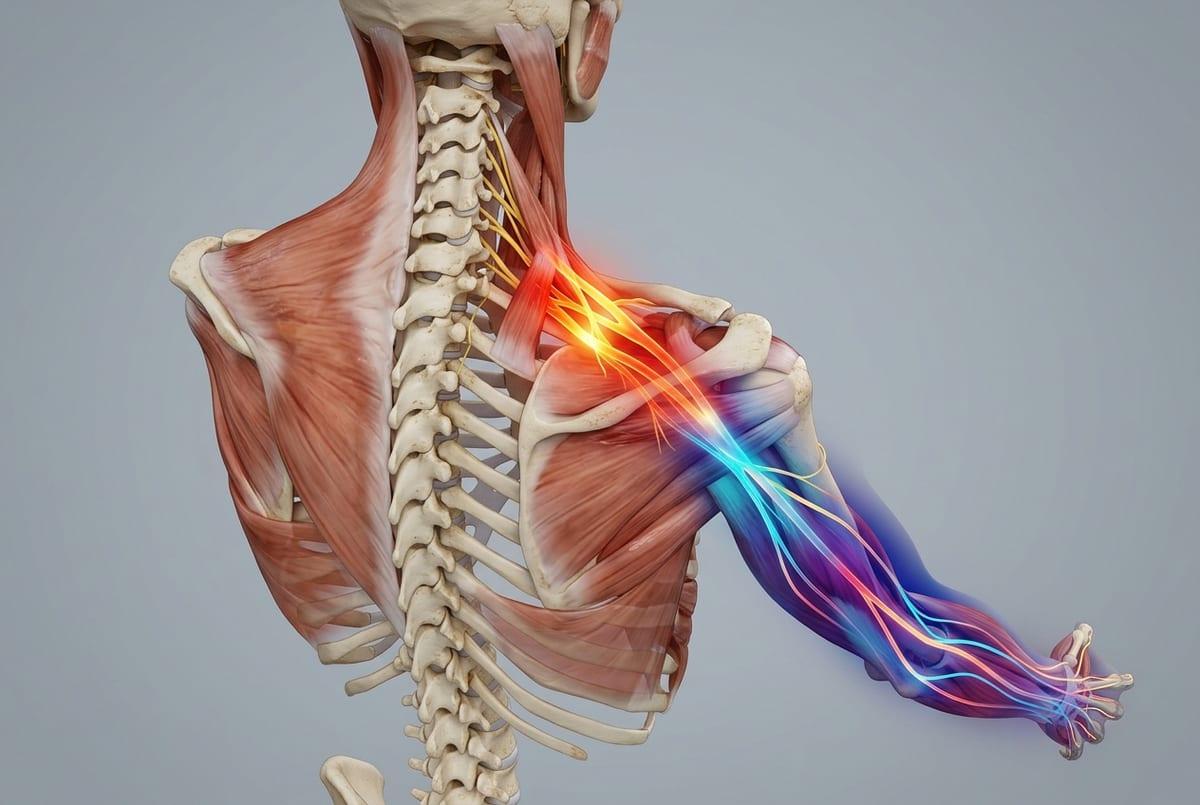
One reason this happens is that the shoulder blade region shares nerve wiring with parts of the arm. Signals from the neck and upper back can converge in the same pathways the brain uses to map sensation down the arm, so the nervous system may interpret irritation in one area as discomfort somewhere else. When this has been building from repetitive posture or load, the system can become more reactive, so a smaller movement—turning the head, reaching forward, sitting tall—suddenly changes the intensity or “direction” of the pain.
The pattern doesn’t always stay consistent. Some days it behaves like a local muscle ache; other days it feels sharper or more traveling, especially when tissues around the neck, upper back, or shoulder girdle are a bit sensitized from overuse rather than a single obvious injury.
Referred pain pathways that mimic an arm problem
At a desk, it can be strange to notice the arm “complaining” when you’re sure the sore spot is under the shoulder blade. You might even start testing the elbow or wrist, because that’s where the ache seems to land—except the tenderness stays anchored higher up.
This is one of the ways referred pain can mislead. Some tissues around the neck and upper back send sensory signals into the same spinal segments that also collect input from the upper arm and hand. When those inputs converge, the brain may not separate them cleanly, so irritation near the shoulder blade can be experienced as an arm problem, even when the arm itself isn’t the main source.
A posture that loads the upper back (rounded shoulders, head angled forward, arms held out in front) may “turn up” the arm symptoms, while local pressure under the shoulder blade feels sore but doesn’t fully recreate the traveling pattern. In some cases, the more the system has been irritated over days or weeks, the easier it is for a small position change to shift where the discomfort shows up.
Nerve irritation and the ‘electric’ traveling sensation
Sometimes it isn’t an ache at all—it’s a quick zap, a hot line, or a “buzz” that seems to run from the shoulder blade area into the upper arm or two fingers. It can show up when you tilt your head, reach to the keyboard, or settle into the car seat, and then disappear just as fast, which makes it hard to trust what’s causing it.
That “electric” quality can happen when a nerve is getting irritated rather than a muscle simply being tired. Nerves are built to carry signals, so when they’re compressed, stretched, or rubbed repeatedly (often near the neck or where nerves pass between muscles), they may start firing more easily. The nervous system can also become more sensitive over time—after days of sustained posture or repetitive loading, the same position that was fine last week may suddenly produce tingling, shooting pain, or a strange cold-and-warm mix down the arm.
It’s also easy to misread this as an arm injury, because the sharpest sensation may land far from the original “bottleneck.” If the traveling feeling keeps expanding, starts coming with noticeable weakness, or doesn’t settle between flare-ups, it’s usually worth getting it evaluated rather than trying to outwork it.
Muscle and joint sources behind the shoulder blade
After a few hours of mousing or carrying a bag, it can feel like there’s a “knot” under the shoulder blade that you can almost press on—yet the arm still gets the louder message. The confusing part is that pushing on the tender spot may recreate a deep, spreading ache, but not the exact fingertip tingling you were tracking earlier.
In some cases, this comes from muscle trigger points in the shoulder-blade stabilizers (often the rhomboids, middle/lower trapezius, or the muscles along the inside border of the blade). Those spots can become irritable when the shoulder blade is held in a slightly strained position for long stretches—rounded shoulders, arms forward, neck subtly jutting—so the muscle’s local chemistry stays “on.” The nervous system can then interpret the input as broader than it is, sending pain into the upper arm even though the muscle itself is the main generator.
Joint mechanics can add to the inconsistency. If the upper back joints or the rib joints under the shoulder blade get stiff or overloaded, the shoulder blade may move less smoothly on the rib cage, and nearby muscles work harder to compensate. That extra effort can make the pain pattern shift day to day—more sharp with reaching one afternoon, more dull and spreading after a long sit—without a single clear injury to point to.
When chest and upper back issues refer pain

It can catch you off guard when the ache flares after something that doesn’t seem “shoulder” at all—like a tight sports bra, a seatbelt pressing across the chest, or a day of leaning into the steering wheel. The discomfort may still land under the shoulder blade, yet the arm feels involved, which can make it tempting to chase the sensation down the limb.
One reason is that the rib joints and upper back joints share close neighborhood wiring with the nerves that also serve the shoulder girdle. If the small joints where ribs meet the spine get irritated, or if the upper thoracic spine is stiff and overworked, the body can interpret that input as pain traveling toward the shoulder blade and into the upper arm. Breathing mechanics can quietly add to it: when the chest wall is held rigid for hours (shallow breathing, braced posture), the same tissues get repeated low-level strain, and the signal can feel bigger than the local spot.
This is also where symptoms can be inconsistent. A deep breath, a twist to check a blind spot, or lying on one side may change the pain more than moving the arm itself—suggesting the “driver” may be closer to the chest or upper back than it first appears.
Relief options that match the likely pain generator
On the days when the discomfort spreads, it’s common to try the one thing that “usually works”—only to find it helps the shoulder blade but not the arm, or calms the tingling but leaves a deep ache behind. That mismatch is often the point: different pain generators respond to different kinds of input, and the same move can feel relieving one day and irritating the next.
If the sensation is more electric or zinging, relief often comes from reducing nerve provocation rather than “digging into” the sore spot. Positions that repeatedly tension the nerve pathway (head tilted, shoulder slightly hiked, arm reaching forward) can keep the nerve reactive, so symptoms may settle more with brief breaks from that posture, gentle neck/upper-back range of motion, or changing how the arm is supported while you work. Deep, aggressive stretching can feel logical but sometimes keeps the nerve on edge.
When it behaves more like a broad, spreading muscle ache, local heat, light pressure, and gradual shoulder-blade movement can be more reliable—because the muscle tissue itself is the louder signal. If the pain clearly changes with breathing, twisting, or rib pressure, it may respond better to thoracic mobility and letting the chest wall move again. If attempts at relief keep producing inconsistent results or the radiation keeps intensifying, that pattern is worth treating as a reason to pause and reassess rather than push through.
Signals that warrant urgent evaluation or imaging
It can be unsettling when a familiar ache suddenly doesn’t behave like it usually does—especially if the arm starts feeling “different” even while you’re sitting still. That change in pattern is often the reason to take the situation more seriously, because irritation that used to be position-dependent can become less predictable as the nervous system stays keyed up.
Signals that are harder to explain away include new or worsening weakness (dropping objects, trouble lifting the arm), numbness that doesn’t come and go, or symptoms that spread quickly beyond the usual area. Pain that is severe at rest, wakes you repeatedly, follows a major fall or crash, or comes with fever or unexplained weight loss may also deserve prompt evaluation, since those patterns don’t fit the typical “overuse and sensitivity” cycle.
It’s also worth treating chest pressure, shortness of breath, sweating, nausea, or pain that feels tight or heavy and isn’t clearly linked to posture or movement as urgent—especially if it’s new for you. If you’re unsure which bucket your symptoms fit into, getting checked sooner is usually the safer call.











