What buttock pain feels like in real life
It can start as a dull, hard-to-place ache you only notice after you’ve been sitting awhile—like you’re perched on a knot. When you stand up, the first few steps may feel stiff or guarded, and then it eases just enough to make you wonder if you imagined it. Later, it can return during a run warm-up or halfway up a flight of stairs, not always in the same spot.
Some people describe it as deep and heavy, almost bruised, centered in one buttock and worse when pressure builds from sitting or a long car ride. Others notice a sharper, more electric or burning feeling that seems to “trace” into the back of the thigh. That mismatch can be confusing, especially when stretching helps one day and irritates it the next.
Part of the mixed signal is that several tissues share the same neighborhood. When a muscle or tendon is slightly overloaded, the body may tighten nearby muscles to protect the area, which can create dense, sensitive trigger points. When a nearby nerve is irritated, the sensation can feel less like soreness and more like heat, zing, or spread—sometimes without a clear injury moment to point to.
Why discomfort appears during sitting, stairs, and running
Sometimes the first clue is how quickly it shows up once you sit: a few minutes can feel fine, then pressure starts to build in one spot, as if the tissue under the sitting bone is getting “pinched.” That pressure can matter because sitting holds the hip in flexion and keeps steady compression on the gluteal tendons and deeper hip rotators, while also reducing the normal, subtle shifting that happens when you’re standing. If those tissues are already a bit irritable, the nervous system may respond with protective tightening, which can make the area feel denser and more tender even without a new injury.
Stairs and running change the problem in a different way. Each step asks the hip to stabilize the pelvis while the gluteal muscles and their tendons manage load and control rotation—especially as you push up or propel forward. After a training jump or a long period of sitting, the workload can land unevenly: a tendon may feel “grippy” or sore with effort, while a nearby nerve can feel more reactive to repeated hip motion, creating a sharper or burning edge. The inconsistency—fine on flat ground, worse on hills or after intervals—often reflects how sensitive that load threshold has become rather than a single structure failing.
Muscle strain, tendon irritation, and deep trigger points
It can feel oddly specific: one spot that’s tender when you press it, and a wider ache that shows up only after you climb stairs or finish a workout. A mild muscle strain often behaves like that—more noticeable with contraction or stretch, and sometimes better once you’re warmed up—yet still inconsistent enough to make you question whether you “did anything” to cause it.
Tendon irritation tends to announce itself differently. Tendons don’t love repeated compression plus load, so the discomfort may build during sitting or side-lying, then flare when the hip has to stabilize under you (stairs, running, single-leg work). Because tendons have a slower, more stubborn irritability pattern than muscle, the next day can feel surprisingly stiff or “grabby,” even if the workout itself didn’t feel dramatic.
Deep trigger points can complicate both. When tissue is irritated, nearby muscles may tighten to limit motion, and that sustained guarding can create a sensitive, knotted band that refers pain outward—sometimes into the back of the thigh. That referral can mimic nerve pain, even when the driver is local muscle and tendon sensitivity rather than a single, clear injury.
When nerves mimic muscle pain and confuse diagnosis
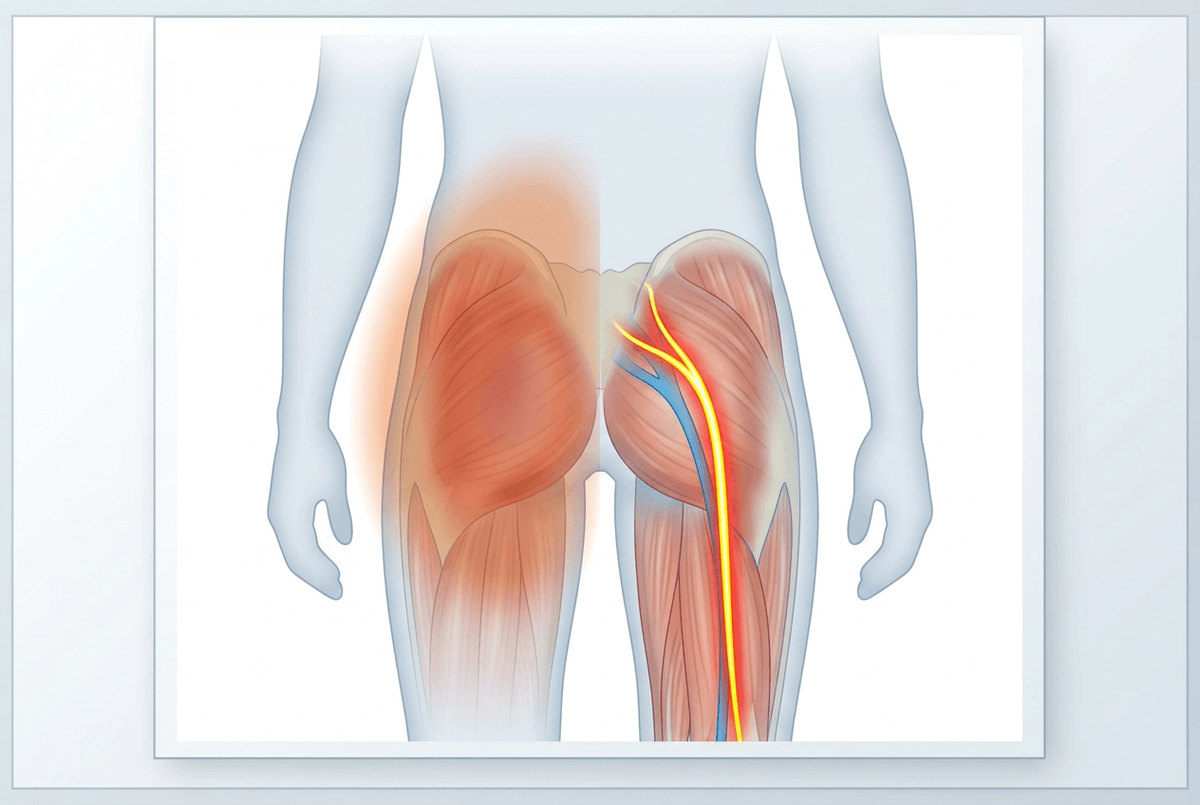
It’s often the “hot line” feeling that throws people off—one day it’s a deep knot in the buttock, and the next it feels like a thin burn that runs into the back of the thigh when you sit or when you hinge forward to pick something up. Because the painful spot is still in the same neighborhood, it can seem like the muscle is simply getting worse, even if the sensation quality has changed.
Part of the confusion is how easily nerves borrow the language of muscle pain. The sciatic nerve and its nearby branches pass close to the deep hip rotators and the hamstring origin, and they don’t need to be “pinched” to get reactive. In some cases, a sensitized nerve fires more readily after steady pressure (like a car seat) or repeated hip motion, and the brain interprets that signal as burning, tingling, or a quick “zap” rather than soreness.
That overlap is why self-tests can feel inconsistent. A stretch or foam rolling may briefly dull a guarded muscle, yet if a nerve is already irritable, the same input can amplify the symptoms and make the pain seem like it’s spreading. If that pattern keeps repeating, it’s worth treating it as a different kind of signal—not just a tighter muscle.
A reasonable stretch that unexpectedly makes pain worse
You lean into a figure‑four stretch and it feels like the “right” spot—until you stand up and the ache has a sharper edge, sometimes with a faint burn down the back of the thigh. That reversal can be unsettling, especially if stretching usually helps your other tight areas.
In some cases, the position that opens the hip also puts the deep rotators and gluteal tendons on tension while the sciatic nerve is asked to glide. If those tissues are already irritated, that extra pull can act less like relief and more like a stronger signal to protect the area. The nervous system may respond by tightening around the hip, which can make the buttock feel denser afterward rather than looser.
A mild stretch may feel fine one day and aggravating the next, depending on how sensitized things are from sitting, hills, or workouts. If a “reasonable” stretch reliably ramps symptoms up or makes them spread, it’s a cue to treat that reaction as information, not a failure of flexibility.
How clinicians narrow causes without overtesting
In the exam room, it’s often the small details that feel surprisingly hard to answer: is the pain worse after sitting or after effort, does it stay in one spot or drift, and does it change from a deep ache to a burn depending on the day. People will sometimes point to one “knot” and assume that’s the whole story, even when the pattern keeps shifting.
Clinicians usually start by mapping the pattern instead of ordering images right away. They’ll look for whether symptoms behave more like a load problem (worse with stairs, running, single-leg work, or after sitting compression), a nerve-sensitive problem (burning, zinging, easier spread, more reactive to positions that tension nerves), or referred pain from the low back or hip (symptoms changing with spine or hip motion more than local pressure). The goal isn’t a perfect label on day one; it’s a working hypothesis that fits the cause-and-effect of your triggers.
Then they try to reproduce and calm it in controlled ways—pressing on specific tendon or muscle regions, checking hip rotation strength, and using movements that bias the spine, hip, or nerve glide. If a test “kind of” matches but not consistently, that uncertainty matters: it can be a sign that sensitized tissue and protective guarding are amplifying signals, so more testing doesn’t always add clarity unless there are red flags or progressing neurologic changes.
Treatment paths that match the likely pain driver
When the pain keeps changing—fine on flat ground, sharp on stairs, then grumpy after a car ride—treatment usually works better when it matches the “driver,” even if the label still feels uncertain. Otherwise you can end up chasing tightness when the real problem is sensitivity to load or pressure.
If it behaves like a workload issue (deep ache, sore with stairs or single‑leg effort, stiff the next day), the path often centers on dialing down the aggravating volume and rebuilding capacity with slower, more controlled hip work. With tendon‑type patterns, too much stretching can feel like effort without payoff, because compression plus load is what tends to keep it irritable.
If it behaves more nerve‑sensitive (burning, zinging, easier spread, worse with positions that “pull”), the focus is often on calming reactivity and avoiding repeated provocation rather than “releasing” the spot. And if symptoms keep escalating, or you notice growing numbness or weakness, it’s a reason to check in sooner rather than later.











