You’ve had a cough for 8+ weeks—what “long enough” changes now
At first, a cough feels like a leftover from a cold that just needs time. You try lozenges, tea, allergy pills, maybe a few nights with a humidifier, and you expect it to fade. When it’s still there at eight weeks, the question changes from “How do I soothe this?” to “What’s keeping it going?”
In adults, a cough lasting 8+ weeks is usually treated as a chronic cough, which means common “maintenance” causes move up the list—post-nasal drip, asthma-related cough, reflux, and medication side effects are frequent examples. It also means your notes start to matter: when it started, what makes it worse, what you’ve already tried, and whether you’ve had weight loss, fever, coughing blood, or shortness of breath.
That’s the point where you stop guessing and start sorting.
Before you troubleshoot: signs that mean you shouldn’t wait for a routine visit

Sorting is useful, but some patterns mean you should stop self-managing and get urgent advice the same day. If you’re coughing up blood (even streaks), struggling to breathe at rest, having chest pain or pressure, or your lips or face look bluish, treat that as an emergency. The same goes for a high fever that won’t come down, confusion, or feeling faint—especially if your cough is getting quickly worse instead of slowly better.
Other “don’t-wait” signs aren’t dramatic, but they change what a clinician needs to rule out. Go sooner if you have unexplained weight loss, night sweats, hoarseness that persists, new swelling in your legs, or you wake up short of breath. If you have a weakened immune system, have heart or lung disease, or you’ve had a blood clot before, the threshold is lower.
It can be hard to describe breathlessness accurately. If you can’t climb one flight of stairs the way you used to, say that plainly—and bring the timeline with you.
What your cough is “telling” you: patterns that make a visit more productive
Bringing the timeline helps, but the details that speed up the visit are usually about pattern. People often say “it’s just all day,” but if it’s mainly overnight, mainly after meals, or mainly with exercise, that points the questions in different directions. Note whether it’s dry or brings up mucus, and if the mucus is clear, yellow-green, or foul-smelling. Also write down whether you hear wheeze, feel chest tightness, or get a “tickle” in the throat that triggers coughing fits.
Triggers are especially useful because they’re easy to test against. Cough that flares with cold air, laughing, or climbing stairs often behaves differently than cough that spikes when you lie flat or after coffee, or spicy food. If you cough more when you talk on the phone, that matters too.
A one-week log—time of day, meals, activity, exposures, and what you tried—can replace guesswork with usable clues.
If it feels like throat drip, wheeze, or heartburn—how common causes get sorted
Those clues get used to separate three very common “lanes” of chronic cough: upper-airway drip, asthma-type airway irritation, and reflux.
If you keep clearing your throat, feel a tickle high in the throat, or notice more cough when you lie down, clinicians often think about post-nasal drip from allergies or chronic sinus irritation. The exam may focus on the nose and throat, and they may try a targeted trial (like a nasal steroid spray) rather than a long list of tests.
If you wheeze, feel chest tightness, or cough with exercise, cold air, or laughing, the questions shift toward asthma or cough-variant asthma. That usually brings breathing tests, and sometimes a short trial of an inhaler to see if the pattern changes. If cough spikes after meals, at night, or with coffee, reflux moves up the list—even without “heartburn.” A real-world catch: these trials take weeks, and overlapping causes are common, so the first plan doesn’t always end it.
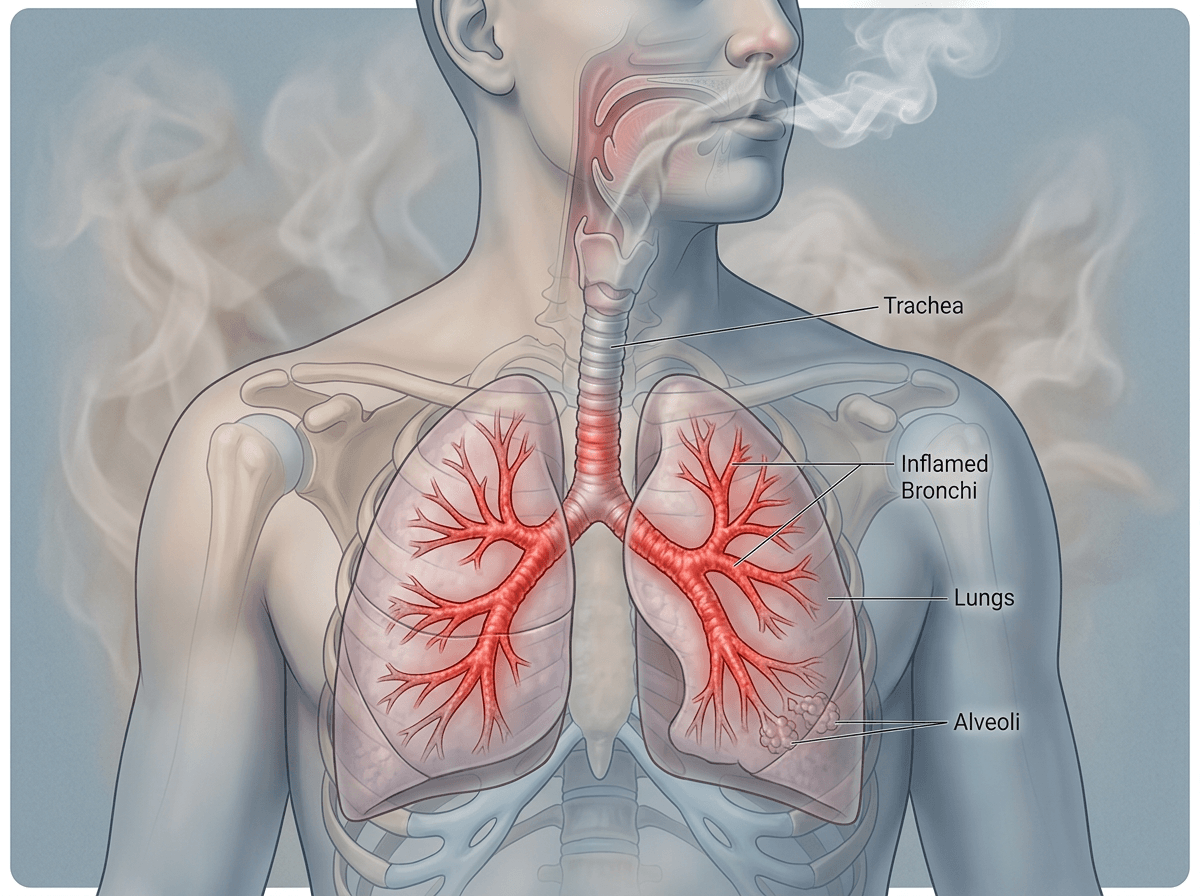
The surprise culprits people miss: medications, smoking/vaping, and sleep-related issues
When the first round of “drip, wheeze, heartburn” fixes doesn’t change much, the cause is sometimes sitting in plain sight. A common one is medication: ACE inhibitors for blood pressure can trigger a dry, nagging cough, even if you’ve taken them for a while. Bring an exact med list, including new drops, supplements, and “as needed” pills, because the solution may be a simple switch—not another inhaler.
Smoking and vaping also keep airways irritated long after the original cold is gone. People often underestimate “just a few hits” or weekend use, and secondhand smoke counts. The hard part is the timeline: cough can briefly worsen after quitting as your lungs clear mucus, so it’s easy to think stopping “didn’t help.”
Sleep can be the hidden amplifier. Snoring, waking with a dry mouth, or reflux when you lie flat can drive nighttime cough, and treating the sleep issue may be what finally makes the pattern budge.
What a clinician is likely to do next—and why tests happen in that order
When a cough keeps hanging on despite the obvious fixes, the visit usually shifts from “try this” to “prove or rule out.” Most clinicians start with the simplest, highest-yield steps: a focused exam (nose, throat, lungs), your medication list, and a chest X-ray if one hasn’t been done since the cough became chronic. That order isn’t about minimizing care; it’s about catching common problems early and not missing bigger ones that don’t announce themselves with dramatic symptoms.
If the X-ray is normal and the story still fits a common lane, the next step is often targeted testing rather than a scattershot workup. Spirometry (breathing tests) helps confirm asthma-type patterns and can show obstruction you can’t feel day to day. If reflux or sinus disease stays high on the list, the clinician may keep using time-limited treatment trials before sending you for a CT scan, scope, or specialty referral.
Each step can take weeks, and insurance rules sometimes require “step therapy” before approving higher-cost tests, which is why a clear timeline and symptom log can speed decisions.
Walking into your appointment with a plan (and leaving with clear next steps)
That timeline and symptom log can also keep your appointment from turning into a vague “still coughing” conversation. Bring a short list: when it started, any “don’t-wait” symptoms you’ve had (even if they passed), what you’ve tried and for how long, and exposures that matter (smoke/vape, new pets, dust, recent travel). Bring your actual medication bottles or a complete list, including blood pressure meds, inhalers, nasal sprays, and supplements.
At the end, ask for three concrete items in writing: what they think is most likely, what they’re ruling out now (and how), and what you should do if it’s not better by a specific date. A common snag is slow follow-through—imaging appointments, prior authorizations, and referral waits—so confirm who orders each test and how you’ll get results.